

Oct 30, 2025

The $1,000 Sleep Challenge
A few days ago, a fitness coach named Ty Woosley made an offer on Twitter: $1,000 to anyone who could permanently fix his sleep.
He hasn't slept through a night in 10 years. He wakes up 8-10 times every single night.
The post exploded.
Over 1.7 million views. More than 6,000 replies. Matt Walker, author of Why We Sleep, offered to help. Bryan Johnson shared his detailed sleep protocol. Thousands of people jumped in with solutions.
At Rest, we've spent years working closely with people navigating the challenging journey of finding sleep solutions. It often feels like the Wild West—conflicting advice, overwhelming options, and no clear path forward. This thread seemed like a unique opportunity to better understand these challenges at scale.
So we analyzed over 1,000 messages. Categorized every recommendation. Counted specific mentions. Looked for patterns. We expected to find some consensus—maybe a few standout recommendations that kept appearing.
What we actually uncovered reveals why solving sleep problems feels impossible in 2025—and what actually works.
52 Different Solutions
Our analysis process was straightforward: we filtered out jokes, spam, and pure empathy responses to focus on actionable recommendations. We then extracted every specific intervention mentioned and counted frequency.
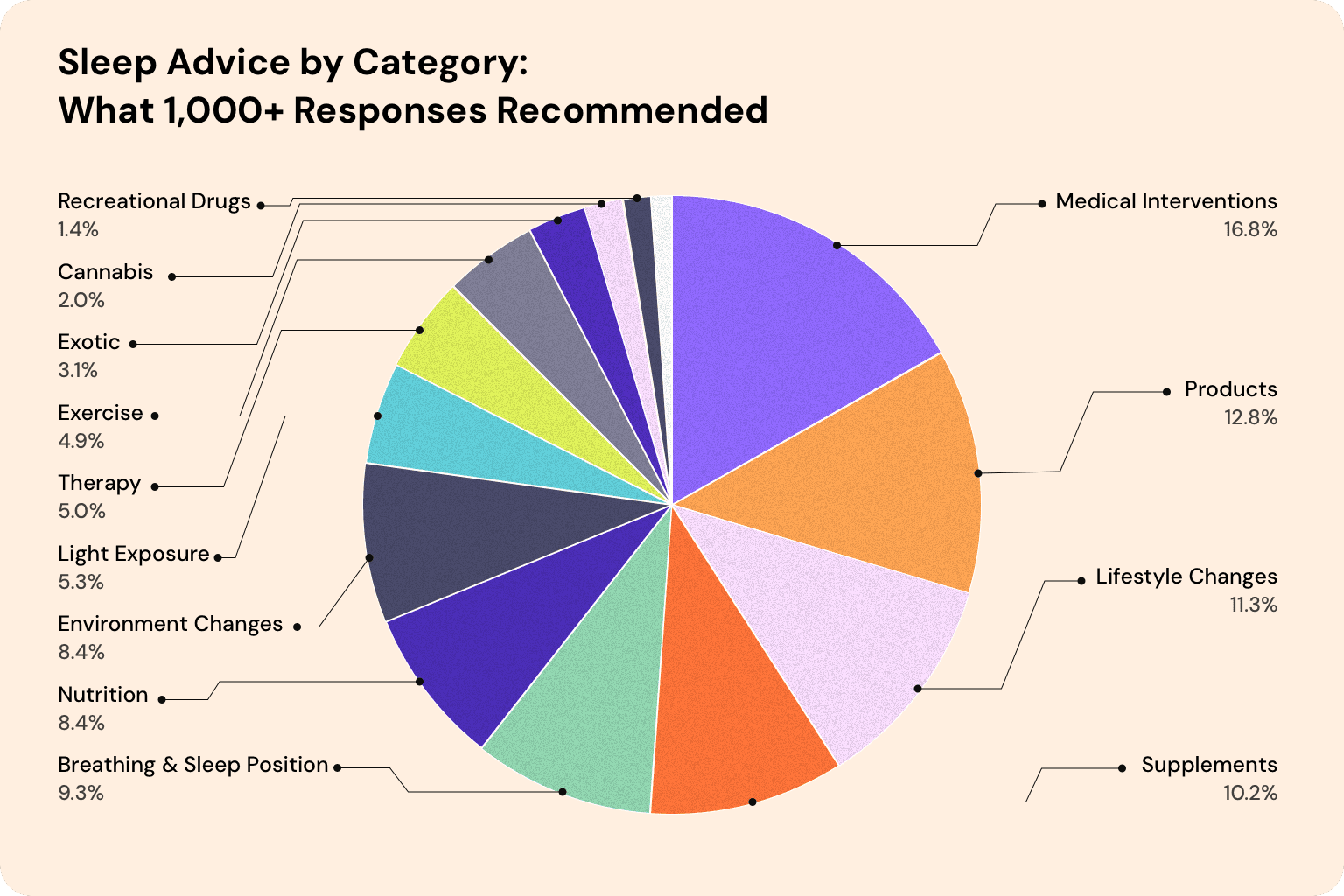
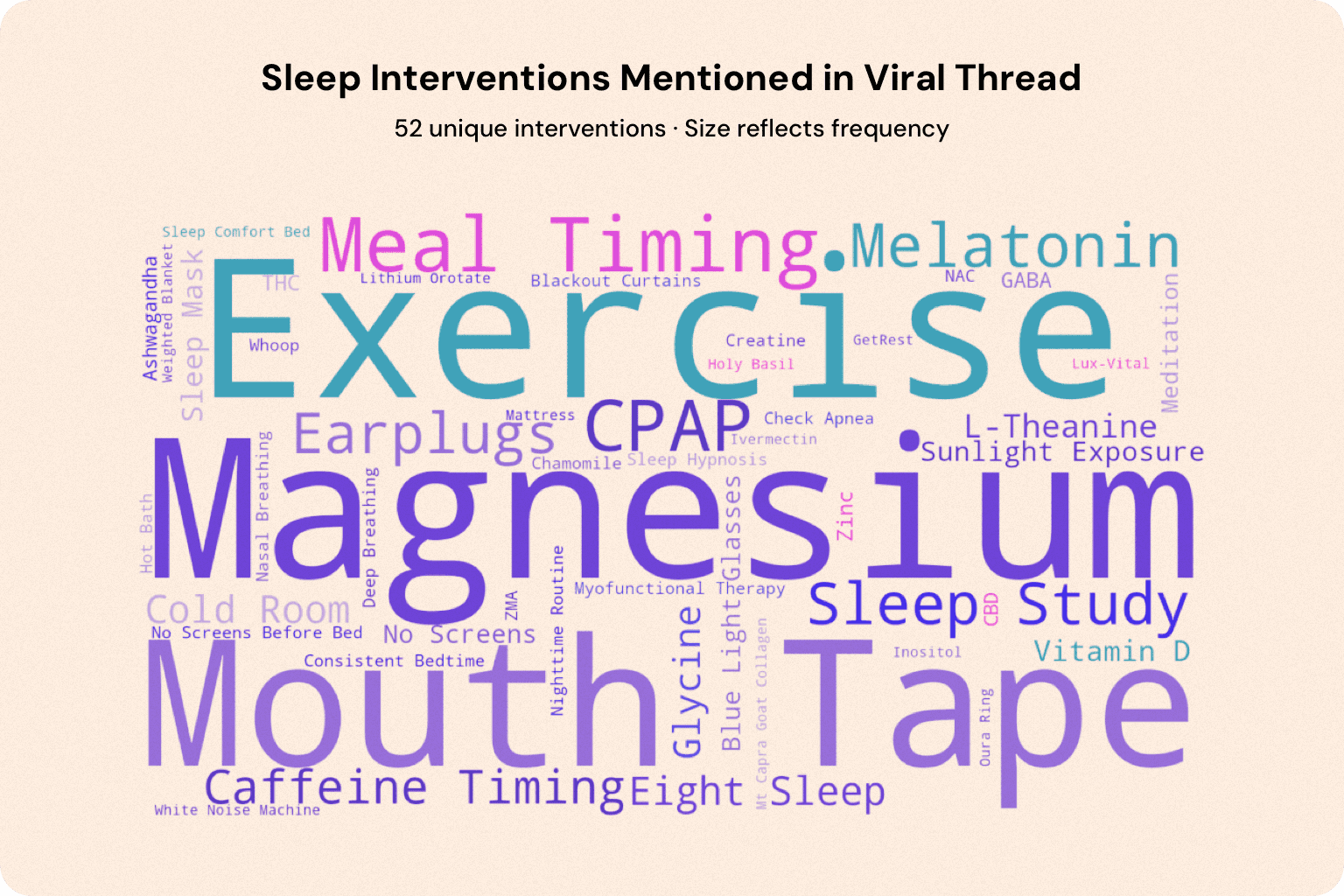
After filtering for interventions with sufficient mentions, we identified 52 distinct interventions:
Supplements (magnesium, melatonin, glycine, L-theanine, GABA, zinc, and dozens more)
Products and devices (Eight Sleep, CPAP, mouth tape, earplugs, blue light glasses)
Medical interventions (sleep studies, prescriptions, testing)
Lifestyle changes (exercise timing, meal timing, caffeine restrictions)
Environmental modifications (room temperature, darkness, noise control)
Breathing techniques and sleep position
Light exposure protocols (morning sun, sunset viewing, blue light avoidance)
Therapy and psychology (CBT-I, hypnosis, meditation)
Spiritual practices (prayer, Bible reading)
Alternative approaches (skydiving, sleeping on boats, and more unusual suggestions)
How is one supposed to make sense of this?
The #1 Sleep Recommendation - Not the Sleep Supplement You Expected
If you asked most people to name a sleep supplement, they'd say melatonin. It's the one everyone knows—the hormone that regulates sleep-wake cycles, available at every pharmacy.
But in our analysis, melatonin wasn't the most recommended intervention.
Magnesium was.
With 58 mentions, magnesium beat out melatonin (28 mentions), CPAP recommendations (38 mentions), and every other intervention in the thread.
However, even with magnesium as the clear frontrunner, people couldn't agree on the specifics.
Which type?
"Magnesium glycinate, along with ashwagandha..."
"Also, consider Magnesium L-Threonate. The specific magnesium type is key"
"Magnesium, all three kinds."
Some insisted glycinate was essential. Others swore by threonate. A few recommended taking multiple types simultaneously.
And melatonin? The confusion was even worse.
How much?
"Try melatonin, 3 mg"
"Natrol 10mg melatonin gummies"
"take 5mg 2 melatonin to sleep or if it's 12mg just 1"
"NAC and Melatonin - 40 mg"
The dosing recommendations ranged from 3mg to 40mg—a more than 13-fold difference. Some recommended time-released formulations. Others said to take it one hour before bed, or two hours before bed.
There's a lot to unpack about magnesium's role in sleep, and melatonin's dosing complexity. But the key takeaway: even the most recommended interventions had no clear consensus on how to actually implement them.
What Rose to the Top
After magnesium and melatonin, what else rose to the top?
Here's what the data showed:
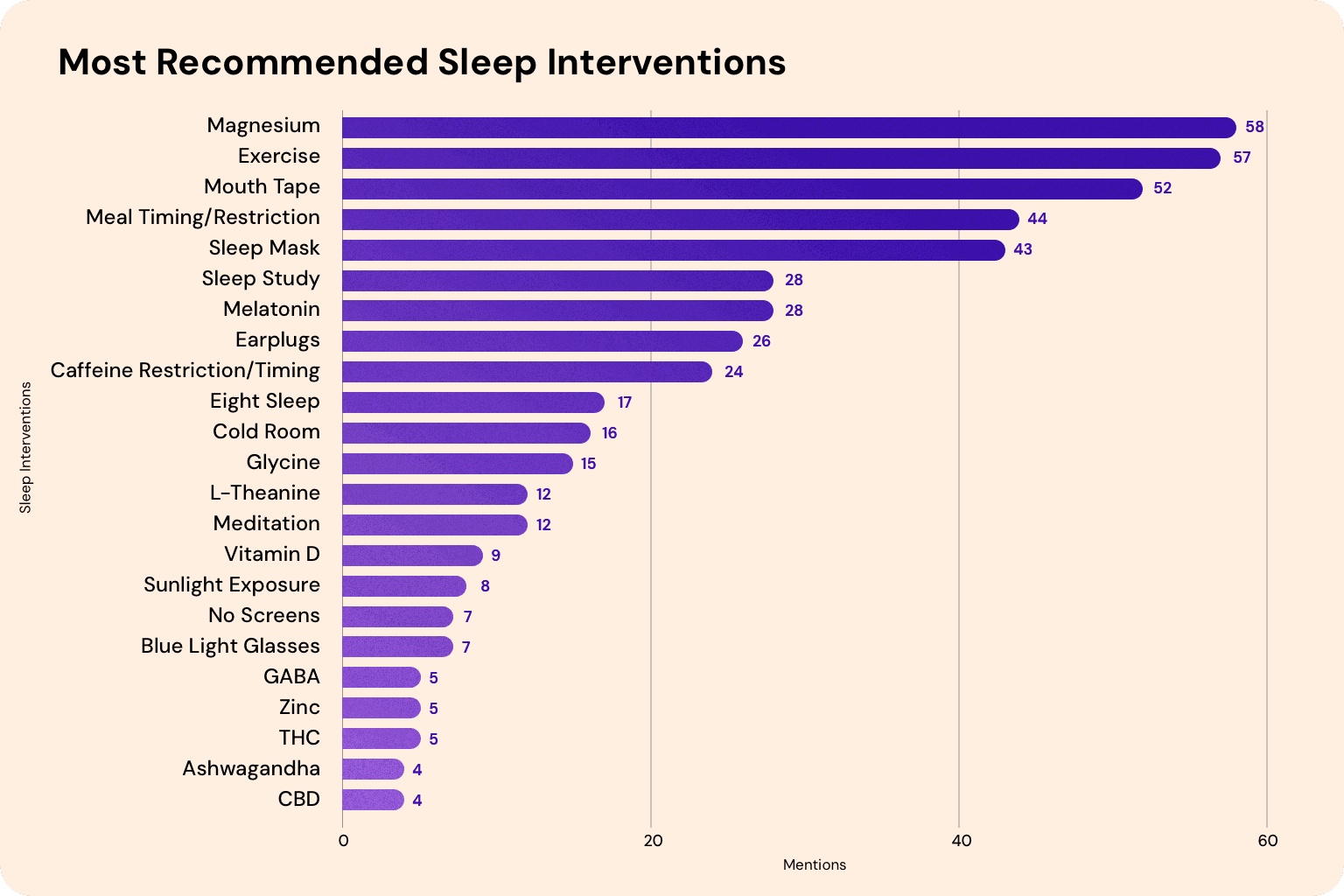
Magnesium - 58 mentions
Exercise (timing advice) - 57 mentions
Mouth Tape - 52 mentions
Meal Timing/Restriction - 44 mentions
CPAP/Sleep Mask - 43 mentions
Sleep Study - 28 mentions
Melatonin - 28 mentions
Earplugs - 26 mentions
Caffeine Restriction - 24 mentions
Eight Sleep - 17 mentions
Some patterns worth noting:
Mouth tape was surprisingly popular, earning 52 mentions—making it more recommended than sleep studies or melatonin. Several people referenced James Nestor's book Breathe as the source of this recommendation.
Exercise timing advice was mixed. Some insisted you should exercise early in the day, keeping it far from bedtime. Others recommended working out close to bedtime specifically to be completely exhausted. Both camps claimed their approach worked.
Meal timing followed the same split. Finish your last meal 2-4 hours before bed, many said. Others recommended eating just before bed. And the dietary advice itself? Some advocated avoiding sugar and carbs entirely. Others specifically recommended loading up on carbs right before bedtime.
Even the more straightforward recommendations came with implementation debates.
This was the top ten. There were 42 more interventions beyond these.
The Long Tail of Sleep Advice
Among the 1,000+ messages, some stood out for sheer creativity:
Skydiving - "The memory of weightlessness brings peace and knocks you out"
Sleeping on a boat - "The rocking motion gives me the best sleep of my life. I think it's the rocking motion"
Eating a block of cheddar before bed - No explanation provided
Shining a bright light behind your knees - "It resets your circadian rhythm"
Ivermectin - "To clear spike proteins from being around vaccinated people" and for "parasite cleanses"
Ecstasy/MDMA - "The best sleep aid known to man, check the article by A Midwestern Doctor"
Some of these were offered with conviction. Others might have been borderline trolling, but it’s hard to say which one is which.
These examples sit outside the 52 interventions with sufficient volume we tracked—they're part of a long tail of exotic suggestions that show just how fringe modern sleep advice can get.
The Impossible Math
The Need for a Methodical Approach
When you're dealing with a persistent problem—like waking up 8-10 times a night for a decade—you need a systematic way to evaluate solutions. Random trial and error wastes time and money, and when you're sleep-deprived, you can't afford either.
So what would a methodical approach to testing these interventions actually look like? Let's focus on the 52 more established sleep interventions we identified—setting aside the exotic suggestions like skydiving and cheddar cheese.
The Math:
Testing each intervention for just 2 weeks to see if it helps: 2 years.
But sleep is complex. And many respondents didn't recommend just one thing—they shared specific combinations, sequences, and protocols:
"Final meal 4 hours before bed, screens off 60 min before bed, same bedtime every day, 60 min wind down, read for 10 minutes, light first thing in the am, final caffeine around noon, liquid intake pushed to earlier parts of the day..."
"Fish oil, pre and pro biotics. Vitamins D3 and magnesium glycinate. Lots and lots of exercise."
Testing combinations of 2 interventions:
1,326 possible combinations
At 2 weeks each: 51 years
And that assumes:
Perfect compliance
No side effects
Unlimited budget
Clear, immediate results
No other life factors interfering
In reality? You'd be lucky to systematically test even 5-10 interventions before exhaustion, confusion, or life circumstances forced you to give up.
The Proven Approach Almost Nobody Mentioned
Here's what genuinely shocked us.
Out of over 1,000 messages analyzed, how many mentioned the methodical approach with an 80% success rate, recommended as first-line therapy by the American College of Physicians and the American Academy of Sleep Medicine?
Three.
We had to triple-check the data because it seemed impossible.
The approach? Cognitive Behavioral Therapy for Insomnia (CBT-I).
It's not just "therapy" or "talking about your feelings." It's a structured, systematic protocol that addresses the behavioral and cognitive factors maintaining insomnia. (You can read our complete breakdown of what CBT-I is and how it works here.)
There is now an overwhelming preponderance of evidence that CBT-I is effective: as effective as sleep medications during acute treatment (4-8 weeks), and more effective than sleep medications in the long term (beyond 3 months after treatment).
Unlike most suggestions in that thread, it targets root causes, not symptoms. The results are durable. It's non-pharmacological. It works within weeks.
Want to learn more about the science? Dr. Ashley Mason, Rest's lead scientific advisor and a leading expert on CBT-I, did an excellent deep dive on Peter Attia's podcast explaining how it works and why it's so effective.
Why the Gold Standard Treatment Got Drowned Out
Why would a treatment with an 80% success rate, didn’t make it into the top 20 suggestions while magnesium got 58 mentions and mouth tape got 47?
1. It's less sexy than biohacks.
"Take magnesium glycinate and use blue light blocking glasses" sounds simpler and more actionable than "Complete a structured 6-8 week protocol that requires tracking your sleep and systematically changing behaviors."
2. Nobody's heard of it.
Despite being the gold-standard treatment, CBT-I has a massive awareness problem. It's not part of the cultural conversation about sleep the way supplements and sleep tracking are.
3. It requires effort.
You can buy supplements on Amazon right now. CBT-I works best with a trained professional or well-designed program. It's not a quick tip you can share in a tweet or a pill you can take.
The Rest Approach: Making CBT-I Accessible
There's another barrier to CBT-I which is access.
Traditional CBT-I treatment has been expensive, often costing thousands of dollars out of pocket. For those seeking insurance-covered options, the wait times can stretch to 1-2 years due to the limited number of trained practitioners.
This is exactly why we built Rest.
We partnered with Dr. Ashley Mason at UCSF and other leading experts—clinicians who learned directly from the creators of CBT-I—to create an AI sleep therapist that makes this science-backed approach accessible.
Rest combines CBT-I with principles from circadian biology and neuroscience to create a comprehensive program designed to fix your sleep in 8 weeks, with many users seeing results in as little as two weeks.
Now with Rest, anyone can get a world-class sleep expert in their pocket, available 24/7 to help them navigate this—without the wait times, without the thousands of dollars, and with personalized guidance that adapts to your specific sleep patterns.
A Better Starting Point
If you're struggling with chronic insomnia—whether it's been 10 years or 10 weeks—here's what the evidence tells us:
Start with CBT-I.
Not as a last resort after you've tried everything else. As your first move.
It's non-pharmacological. It works within weeks. The results last. It addresses root causes, not just symptoms.
Yes, sleep hygiene matters. Your environment matters. Light exposure and exercise timing can help.
But these are secondary to addressing the core behavioral and cognitive patterns that maintain your insomnia.
You don't need 1,000 suggestions across 52 interventions.
You need one systematic approach that works.
Ready to get started?
Rest makes CBT-I accessible, affordable, and personalized to your specific sleep challenges. Built with leading sleep researchers, backed by decades of clinical evidence, designed to get you results in weeks, not years.
Disclaimer: Rest is a self-management and well-being tool for sleep improvement and is not intended to diagnose, treat, cure, or prevent any disease. It does not replace care by your healthcare provider or any treatments you may be using. Always continue to take your medications as directed by your healthcare provider. The information provided in the Rest app and related materials is intended for your general knowledge only and is not a substitute for professional medical advice or treatment for specific medical conditions. Use Rest only as directed. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition. If you have or suspect you have a specific medical condition or disease, please consult your healthcare provider before using the Rest program.
Company: Evolve Global, Inc.